
Measles Outbreak 2019
Katrina Hancock • May 20, 2019
Measles Outbreak 2019: Notes For Healthcare Professionals

Currently, over 800 individual cases of measles have been confirmed in 23 states as of May 10th, 2019. Out of these cases, 6 have been confirmed in Georgia, and the majority (80%) noted from New York.
History: Measles was once a deadly childhood disease in America until the vaccine was created and administered in 1963. The highly contagious childhood infection, which is caused by a virus, is considered extremely rare. In 2000, the measles virus was declared “eliminated” from the United States.
According to the Mayo Clinic, measles spreads when an infected individual coughs, sneezes or talks near other people. Infected droplets from the individual with measles can spray into the air or land on a surface and these droplets can remain active and contagious for hours. Those who are unvaccinated, travel internationally to developing countries or have a vitamin A deficiency are more likely to catch the disease.
Symptoms: Measles typically appear between 10 to 14 days after a person has been exposed to the virus. The symptoms include fever, dry cough, runny nose, sore throat, conjunctivitis, tiny white spots with bluish-white centers on a red background inside the inner linking of the cheek, and a skin rash. In the first 10 to 14 days after an individual is infected, they will show no signs or symptoms of the disease, as the virus is incubating. Then, for two to three days, the person will begin to experience a mild to moderate fever, persistent cough, runny nose, sore throat and inflamed eyes. Infected individuals will then see a splotchy red rash spread, first on the face, then down the body. As the rash spreads, a person can also experience a spike in temperature, according to the Mayo Clinic.
To minimize the risk of measles transmission in healthcare settings, healthcare personnel should:
1. Question patients with a febrile rash illness about if they have of traveled internationally, came in contact with foreign visitors, or had possible exposure to a measles patient in the last 3 weeks.
2. Mask suspect measles patients immediately, if feasible, or loosely cover the heads of infants or young children with a blanket during transport.
3. Healthcare personnel should be up to date with immunizations. Be sure to have had 2 doses of MMR vaccine or laboratory evidence of immunity (measles IgG positive).
4. An N95 respirator mask should be worn by ALL Healthcare personnel, especially the providers that have not completed the immunization series or the titer (N95 respirator must be fit-checked each time it is donned).
5. Notify any location where the patient is being transferred to for additional clinical evaluation or laboratory testing about the patient’s suspected status.
6. Clean the patient area (truck) thoroughly after patient care is transferred.
7. If measles is confirmed in the suspect case, exposed responders will need to be assessed for measles immunity.
Author: Katrina Hancock
Connect with us

The body content of your post goes here. To edit this text, click on it and delete this default text and start typing your own or paste your own from a different source.
February is Black History Month, a time to celebrate the achievements, contributions, and rich history of Black individuals who have helped shape our world. At Faithful Guardian Training Center (FGTC), we take this opportunity to recognize the invaluable impact that our instructors, students, and professionals of color have on the field of emergency medical services (EMS) and beyond. The Importance of Black History Month Black History Month is not just about looking back—it’s about recognizing the present and shaping the future. The legacy of Black trailblazers in healthcare, emergency medicine, and public safety serves as an inspiration for future generations. From Dr. Charles Drew, who revolutionized blood plasma storage, to the many Black EMTs and paramedics serving their communities today, this month is a reminder of resilience, excellence, and progress. FGTC’s Commitment to Diversity and Inclusion At FGTC, we are committed to fostering an inclusive environment where all students and instructors, regardless of background, feel valued and supported. We celebrate the diversity of our staff and students because we know that different perspectives strengthen our ability to serve communities effectively. Our mission is to provide high-quality training for all individuals pursuing a career in emergency medicine. By creating an educational space that promotes equity and opportunity, we empower all our students to thrive in the EMS profession. Recognizing Our Instructors and Students of Color We are proud to have a diverse team of experienced instructors and dedicated students who bring unique experiences and perspectives to our training programs. Their contributions not only enhance the learning environment but also help shape the future of EMS by ensuring compassionate and skilled professionals serve communities across Georgia and beyond. FGTC stands with our instructors and students of color, acknowledging their hard work, dedication, and the barriers they may have had to overcome. Their resilience and passion continue to inspire us all. How You Can Celebrate Black History Month While Black History Month is a time for reflection, it is also a time for action and learning. Here are some ways you can honor and celebrate this important month: ✔️ Educate Yourself – Learn about Black medical pioneers and EMS professionals who have paved the way. ✔️ Support Black-Owned Businesses – Find and support local Black-owned businesses in your community. ✔️ Engage in Conversations – Speak with colleagues and peers about the importance of diversity and inclusion in healthcare and EMS. ✔️ Attend Events – Participate in local or virtual Black History Month events and discussions. ✔️ Mentor and Inspire – If you're in the field, take time to mentor aspiring EMTs and paramedics from underrepresented communities. Moving Forward Together At FGTC, we believe that representation matters. As we continue to train and equip the next generation of emergency responders, we remain dedicated to fostering an inclusive and supportive learning environment for all. This Black History Month, we reaffirm our commitment to diversity, equity, and the success of every student and instructor in our program. Join us in celebrating Black history, not just in February, but every day. Together, we can create a stronger, more united EMS community that serves all people with compassion and excellence. #BlackHistoryMonth #EMSdiversity #FGTC #CelebratingExcellence

Every February, we recognize American Heart Month, a time dedicated to raising awareness about cardiovascular health and the importance of preventing heart disease. As one of the leading causes of death worldwide, heart disease affects millions of people, but the good news is that many risk factors are preventable through lifestyle changes and education.
Why American Heart Month Matters
The American Heart Association (AHA) and other health organizations use this month to emphasize the significance of heart health and encourage people to take proactive steps toward reducing their risk of heart disease. Heart disease doesn’t just affect older adults—people of all ages, including young adults, can develop risk factors such as high blood pressure, obesity, and diabetes. That’s why it’s crucial to spread awareness and take action early.
How You Can Protect Your Heart
Taking care of your heart doesn’t have to be overwhelming. Small, consistent changes in your lifestyle can have a major impact. Here are some way
The staffing shortage in the field of Emergency Medical Services (EMS) is a growing concern that has the potential to impact the health and well-being of communities across the country. EMS professionals, including paramedics and emergency medical technicians (EMTs), play a critical role in responding to medical emergencies and providing life-saving care to patients. However, many EMS agencies are struggling to recruit and retain enough qualified staff to meet the demand for their services. One of the main reasons for the staffing shortage is a lack of funding. EMS is often underfunded, which can lead to low wages and insufficient resources. This can make it difficult for agencies to attract and retain talented professionals. Another factor contributing to the staffing shortage is the high levels of stress and burnout that EMS workers often experience. The nature of the work can be physically and emotionally demanding, and many EMS professionals struggle with mental health issues as a result. The staffing shortage has serious consequences for the communities that rely on EMS services. When there are not enough staff members to meet the demand, response times may increase, and patients may not receive the timely care they need. To address the staffing shortage, EMS agencies need to prioritize investing in their employees. This includes offering competitive wages and benefits, providing support for mental health and well-being, and investing in ongoing training and professional development. In addition, it is important for EMS agencies to work with local governments and community organizations to advocate for increased funding and support. By working together, we can ensure that EMS professionals have the resources they need to provide the best possible care to patients. Overall, the staffing shortage in EMS is a complex issue that requires a multifaceted approach. By supporting and investing in EMS professionals, we can help to address this critical shortage and ensure that communities have access to the vital services they need.

Faithful Guardian Training Center is more than just a school, it is a community. From our staff to our amazing students, we all have the same goal, to reach out to society and make a difference. We work hard at Faithful Guardian to train people to become EMTs, Paramedics, and Firefighters. When they leave our program, they leave with more than just a certificate. They leave with a sense of community, a sense of pride for what we do, and sense of family. While we are not as big as a university, we have staff and students who work hard day and night to succeed and make a difference. I speak from experience on both sides. As a student, I receive all of the resources and help I could possibly ask for to become a successful health care professional. My instructor works morning, day, and night to make sure I have the tools and resources I need to be not only a good EMT but a great one. My administrators work morning, day, and night, to make sure that I am always on the right track. We are given the opportunity to receive practice as third ride students on the ambulance. We are given an infinite amount of resources to study and prepare for National Registry. We are provided with the tools used in the field to practice skills and learn to use them before we get on a truck. I am not only given an education, I am given a team to help me build a career. Not only do I attend classes at FGTC, but I have the privilege to work closely with all of the amazing staff. Though my job is small compared to the hard work of our administrators and instructors, it is amazing to see how our offices work with people to reach their goals. Katrina, our Clinical Coordinator, answers phone calls and emails all day and all night to make sure each and every student gets to experience real time practice at an ambulance service, ensures our safety during our third rides, and makes sure that we enjoy ourselves while doing it. Jordan, our director of operations, answers every little question anyone could ask about our program. She is the know all-tell all of our office and I assure you, if you were to ask her a question about anything that involves our school, she could give you an answer right on the spot. She is the advocate for our students and ensures they are all content with the education and resources they are receiving. Jen, our Program Director, manages to find instructors and ensures that the classrooms are well equipped with people who have the knowledge to expand our minds and teach us how to be successful EMS Professionals, all while teaching a class of her own. So join our team, our family, our community. Know that when you register for our classes you are not just given an education, you are given a family to stand behind you as you start a new and exciting chapter of your life. You are given a meaningful and fulfilling career where no one day in the office is the same and you have the opportunity to make a difference in someone else’s life. We invite you to join, with open arms, in hopes that we can help you achieve your goals.

FGTC would like to shine some light one of our local hospital partners during this trying time to show just how much they go above and beyond for community and students, even outside of these critical circumstances. We appreciate the sleepless nights and endless dedication that these nurses and doctors are putting in to help everyone through the COVID-19 crisis at hand. Thank you! This is a testimony of feedback that we received from one of our current paramedic students after attending an ER rotation at Tanner- Higgins General Hospital in Bremen, Georgia just a short while ago. “I had the opportunity to attend a shift at the ER in Higgins recently and the staff was amazing. I jumped right in like I was at work when I arrived at 7 a.m. I knew most of the employees that were there that day due to previous interactions while working on the trucks at a local ambulance service. Because of this, I didn’t have a specific nurse to follow so I had plenty of opportunities to learn. The ER was busy and I was able to obtain multiple check offs and perform a bunch skills. All of the nurses were kind and eager to let me help and would even wait for me if I was helping another nurse with something at the time if they had something I might not see on the truck. While attending this clinical, we had an arrest that came into the ER that we ended up working for 2 hours and 42 minutes before we were able to stabilize and transfer them to a Cath Lab. Specifically, I want to commend two nurses that I had the opportunity to work with, Kenny and Amy. During this time, and really the entire day, I was treated like a team member and they expected the same professional care and level of knowledge that they had. I was available when the arrest report came in and was waiting in the trauma room when the patient arrived. I fell right into the flow of things rather than feeling like I needed to be instructed on how to run a code. I appreciated that I was treated as a competent provider and they were willing to work right alongside me. They made sure that I had all of the equipment, supplies, and help available when I was performing a skill and they would ask if I needed to swap out if I was becoming tired while performing compressions. They let me administer medications and perform cardiac defibrillation when needed. They were willing to answer all my questions with informative answers and gave both textbook and real world experience point of views. The doctor spoke to me as a team member and would designate tasks as he would his ER staff. When the doctor would ask for recalls and suggestions, I actively and informatively engaged in team conversations and was not taken for granted just because I was a student. At the end of my shift, the doctor and nurses told me I did a great job and would love to have me back again. I would just like to pass along my gratitude and give recognition to the two staff members that really had a positive impact on me. It was definitely a great experience that I will cherish for a lifetime.” -Carly Ragsdale
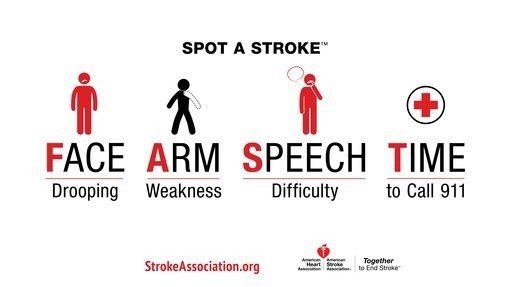
Have you ever been concerned of what to look for if you think you’re having a stroke? The following signs and symptoms to look for are as follows: Additional Signs and Symptoms: • Sudden Numbness- Sudden NUMBNESS or weakness of face, arm, or leg, especially on one side of the body. • Sudden Confusion- Sudden CONFUSION, trouble speaking or understanding speech. • Sudden Trouble Seeing- Sudden TROUBLE SEEING in one or both eyes. • Sudden Trouble Walking- Sudden TROUBLE WALKING, dizziness, loss of balance or coordination. • Sudden Severe Headache- Sudden SEVERE HEADACHE with no known cause. Immediate treatment may minimize the long-term effects of a stroke and even prevent death. Thanks to recent advances, stroke treatments and survival rates have improved greatly over the last decade. A stroke occurs when a vessel in the brain is blocked by blood clots or ruptured vessels. A stroke caused by a clot is called an ischemic stroke, making up about 85 percent of all strokes in the US. Alternate Stroke Treatment Options An endovascular procedure is a treatment to remove the clot by sending a catheter to the site of the blocked blood vessel in the brain. Patients must meet certain criteria to be eligible. Sometimes these procedures involve tPA being administered directly into the blood clot (called intra-arterial treatment) to help dissolve the blockage. In other procedures, the doctor may attempt to remove the clot. Over the last several years the American Heart Association has submitted several resources available to individuals regarding strokes. For more information from the American Heart Association please visit: https://www.strokeassociation.org/en/about-the-american-stroke-association/american-stroke-month .

What is considered high blood pressure? High Blood Pressure is when your blood pressure, force of blood flowing through your blood vessels, is constantly too high. Two years ago, new guidelines from the American Heart Association, the American College of Cardiology, and nine other health organizations lowered the numbers for the diagnosis of hypertension (high blood pressure) to 130/80 millimeters of mercury (mm Hg) and higher for all adults. The previous guidelines set the threshold at 140/90 mm Hg for people younger than age 65 and 150/80 mm Hg for those ages 65 and older. his means 70% to 79% of men ages 55 and older are now classified as having hypertension. That includes many men whose blood pressure had previously been considered healthy. According to the American Heart Association nearly half of the adults in America now have High Blood Pressure. If you didn't have high blood pressure before, there's a good chance you do now. You may not feel that anything is wrong, but high blood pressure could be quietly causing damage and can threaten your health. The best prevention is knowing your numbers and making changes that matter in order to prevent and manage high blood pressure. High blood pressure (HBP, or hypertension) is a symptomless “silent killer” that quietly damages blood vessels and leads to serious health problems. While there is no cure, using medications as prescribed and making lifestyle changes can enhance your quality of life and reduce your risk of heart disease, stroke, kidney disease and more. Make changes that matter: • Eat a well-balanced diet that's low in salt • Limit alcohol • Enjoy regular physical activity • Manage stress • Maintain a healthy weight • Quit smoking • Take your medications properly • Work together with your doctor References for High Blood Pressure, Provided by the American Heart Association: https://www.heart.org/en/health-topics/high-blood-pressure/changes-you-can-make-to-manage-high-blood-pressure https://www.heart.org/en/health-topics/high-blood-pressure/the-facts-about-high-blood-pressure https://www.heart.org/en/health-topics/high-blood-pressure
“When a man becomes a fireman his greatest act of bravery has been accomplished. What he does after that is all in the line of work.” -Edward F. Croker 343… 343 is a number Americans are quite familiar with. 343 is the number of firefighters and paramedics that were killed in the line of duty on September 11th, 2001. That number is still climbing due to cancer and other disease they have developed post the 9/11 attacks. New Jersey Governor Phil Murphy signed two laws Monday enhancing protections for first responders, including those who volunteered for 9/11 rescue, recovery, and clean-up efforts at World Trade Center sites. A4882, also known as "The Bill Ricci World Trade Center Rescue, Recovery, and Cleanup Operations Act," is named after Lieutenant Bill Ricci, a professional firefighter in Clifton who volunteered to serve at Ground Zero after the terrorist attacks on September 11, 2001. Ricci was ineligible for an accidental disability retirement under previously existing law, but through this act, members and retirees who volunteered after 9/11 will be eligible to receive accidental disability retirement. The act also creates an exception to the normal five-year filing requirement for 9/11-related operations. "Thousands of courageous volunteers put their lives on the line in order to save those affected by the devastation of 9/11," Murphy said. "We will never forget their selfless acts of heroism, just as we will always be grateful for the first responders who put their lives on the line for us every day. Today we send a clear message to all of our heroes: We have your back. I am proud to sign legislation that will ensure the health benefits and compensation that these incredible men and women deserve." S716, also known as "The Thomas P. Canzanella First Century First Responders Protection Act," is named after Deputy Chief Thomas Canzanella, a former Hackensack firefighter and advocate who served at Ground Zero after 9/11. Canzanella, who was an International Association of Fire Fighters state representative, passed away from a heart attack at the age of 50. Author: Jade Chasse

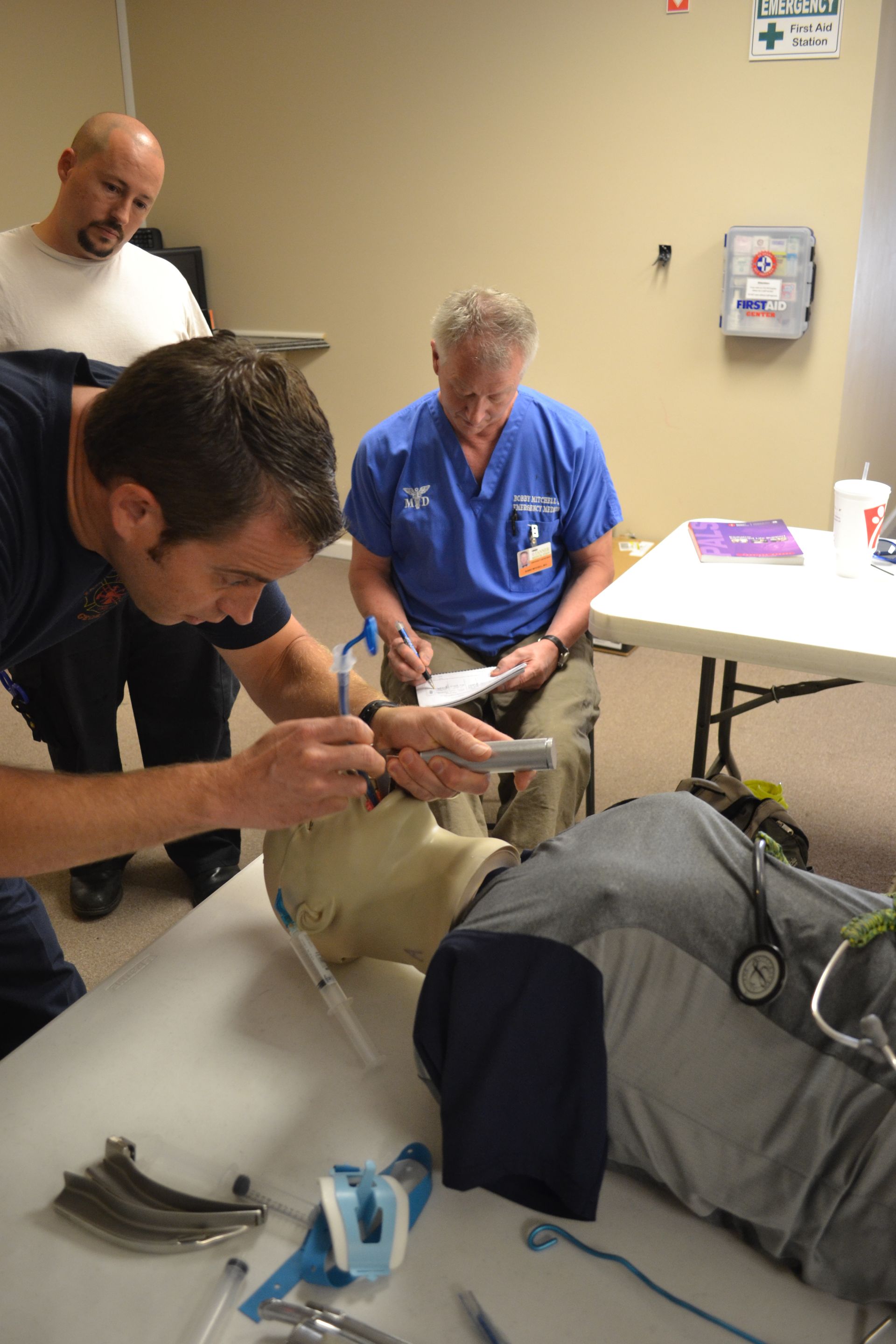
According to “jems” Just 5–15% of patients treated with standard CPR survive cardiac arrest, revealing a need for improved technique. To address this need, mechanical compression devices have become more prevalent and continue to evolve. The LUCAS device has been shown to improve quality of chest compressions, increase ETCO2 levels as well as being able to sustain life-saving circulation during prolonged resuscitation attempts. LUCAS has been studied extensively, shown to be safe and effective and to save patients that would otherwise have been considered futile. There are more than 24,000 LUCAS devices in use today; more than any competitive device. With more than 15 years of experience in automated resuscitation and over 200 studies published, you can rely on LUCAS’ to perform all the way from the site of the emergency to the hospital. Minimum Interruptions- Humans tire and need to frequent rests to maintain good CPR compressions. Transfers from scene to ambulance to stretcher to bed all require interruptions in CPR. Having a fixed, consistent device providing constant compressions is ideal. Reduction of Stress- Treating a victim that requires CPR is stressful enough. Any simplification to the entire ordeal is welcome. Using the LUCAS, responders can focus on other aspects of treatment and not have to constantly wonder who will be relieving them. Removing compressions from the list of things to worry about allows rescuers to deal with the condition causing distress. Fewer Hands Required- If you are short staffed, treating a patient in distress can be even more challenging. Having your teammate, LUCAS, there doing “his” job allows you to focus on other aspects of the rescue. Consistency Saves- The LUCAS automated CPR allows consistent rate and depth of compression, while reducing dangerous interruptions to compressions. Also, the quality of the compressions needed to sustain blood flow is not compromised due to the natural fatigue for emergency personnel. There have been several published accounts of multi-hour (wow!) rescues resulting in the successful resuscitation of patients. Author: Jade Chasse